Photodynamic Therapy
Systemic and interstitial photodynamic tumour therapy
Photodynamic therapy (PDT) is one of the most interesting and promising treatment approaches in the therapy of many different cancer diseases. The principle is the stimulation of a light-sensitive substance based on natural chlorophyll (photosensitiser), which is given into the bloodstream intravenously and (or) injected locally into the tumour. The sensitiser binds to any type of tumour cell in the organism with very high specificity. After stimulation with (laser) light, these are destroyed through the formation of active oxygen radicals. As a rule, photosensitisers are made up of porphyrin molecules or similar structures and are usually derivatives of haem or chlorophyll. Correspondingly, they are known as haematoporphyrin or chlorin. The most modern and selective photosensitzer at present is Chlorin E 6 from the company Apocare in Bielefeld, Germany, which we use exclusively.
Lately, it is known that traditional chemotherapy means also work as photosensitisers, and are considerably stimulated through light-specific wavelengths. So, chemotherapy can be combined with chlorine therapy in low, non-harmful doses.
A particular advantage of the therapy, as opposed to traditional chemotherapy, is that the immune system is not put under stress, but instead is strengthened by the intravenous laser therapy in the after treatment, whereby there is an additional secondary immunisation effect of the photodynamic therapy (PDT-immunisation).
Application:
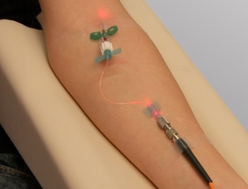
Initially, the sensitiser is infused for 30 minutes and parallel to this, the blood is irradiated with the appropriate absorption wavelength (660 nm red light).
Then follows a 30-minute green laser irradiation session of the blood with simultaneous intravenous oxygen infusion (Oxyven device, Germany), as well as a 30-minute blue laser irradiation session.
For particular tumour diseases, a parallel low-dose chemotherapy is recommended, whereby the chemotherapeutics, such as 5-FU or Cis-Platin, also have a photosensitiser effect and are considerably boosted by the intravenous laser stimulation, despite the low dosage, without putting substantial pressure on the immune system. Here, traditional oncology meets modern low-level laser medicine.
Around 3.5 hours after the chlorin injection, the substance is fully bound to the tumour and this is then locally irradiated externally.
For tumours that are situated deeper, the chlorin can be also injected directly into the tumour (ideally guided by ultrasound) in order to directly irradiate the malign tissue interstitially using a fibre optic catheter. Gastrointestinal tumours (oesophageal, stomach or bowel cancer) can be treated appropriately using an endoscope.

1) Patient with tumour in the stomach area

2) Injection of Chlorin E6 into the blood stream
3) Distribution of Chlorin E6 in the blood stream

4) Accumulation of the Chlorin in the tumour tissue
5) Activation of Chlorin E6 through intravenous and
interstitial laser therapy with additional intravenous oxygen therapy

6) Destruction of the tumour tissue and excretion of the Chlorin E6